
 српски
српскиAchalasia
Achalasia is caused by disordered functioning of the body of the esophagus and sphincter (circular muscle) located between the esophagus and the stomach, which is called the lower esophageal sphincter (LES).Swallowing induces LES to relax and food normally passes from the esophagus into the stomach.In achalasia, lower esophageal sphincter maintains a constant pressure, and does not relax during the passage of food and fluids, which causes the feeling of dysphagia.Food and fluid build up in the esophagus and patients often regurgitate or vomits contents or undigested mouthfuls of food.Over time, the esophagus dilates, which exacerbates the sense of stagnation of food behind the breastbone.An additional problem in patients with achalasia represent a lung damage, which is usually in the form of pneumonia due to the continuous overflow of the contents out of the esophagus into ti windpipe.
Though the exact mechanism of development of achalasia is still not known, it is considered that achalasia is likely the result of a viral infection which leads to damage of the nerve cells in the wall of the esophagus.It was also noted that often occurs in people after the episode of acute or chronic stress.Difficulty swallowing is an alarming symptom that requires mandatory medical consultation.If difficulty swallowing lasts a long time, your doctor may suspect achalasia and introduce you to a series of diagnostic tests to confirm the diagnosis.
Achalasia is a benign functional disorder of the esophagus that leads to difficulty swallowing and if diagnosed in time can be very successfully treated, usually surgically, without further consequences on the health of the patient.
For details about the frequency, causes of, symptoms and methods of diagnosing achalasia please read below.
Introduction
Achalasia (in Greek “inability to relax”) is a disease of unknown cause in which there is loss of esophageal peristalsis and lack of adequate relaxation (relaxation) of the lower esophageal sphincter (DES).Although both of these disorders affect inadequate emptying of the esophagus, the primary symptoms of achalasia (difficulty swallowing and regurgitation) occurring due to the inability of DES to adequately relax.The impossibility of adequate relaxation DES leads to functional obstruction of the esophagus that exists until the hydrostatic pressure of retained content not overcome the pressure that creates muscle DES.
Achalasia was first recognized as a distinct clinical entity still about 300 years ago.This disease is called primary cardiospazam, which recognize functional obstruction of the esophagus at the level of DES.In developed countries, the incidence of achalasia today is 1.5 / 100,000 while its prevalence, considering that the disease is chronic and 11 / 100,000.The last two decades there is a steady increase in the prevalence of the disease.Although regional variations are described in the United States and Europe, not proven the existence of differences related to race or gender.Most patients are diagnosed in živodnom period of 20 to 70 years.It is interesting to note that there is a specific incidence related to the patient so that it occurs or achalasia in young people between 20 and 40 years of age or later in life, at the age of 60 years.The incidence of achalasia is extremely rare before adolescence (5%), but increased with age and was highest for patients in the seventh decade of life.
Causes
Achalasia today represents about 80% of all esophageal motility disorders and their method of formation can be primary (idiopathic) or secondary disease.The cause of inflammatory neuronal damage in patients with primary achalasia is not known.Some findings suggest that achalasia can basically be an autoimmune disease or can result from chronic infection with herpes zooster or measles.Other possible causes of achalasia can be stress, bacterial infections or genetic inheritance.
In patients with achalasia cause damage to the nerve cells of the esophagus for unknown reasons.The loss of nerve cells in the esophagus leads to two basic problems affecting the proper swallowing food and liquids:
- The muscles of the esophagus is not collected properly, so the swallowed food does not move normally through the esophagus into the stomach.
- The lower esophageal sphincter (DES) does not relax properly.
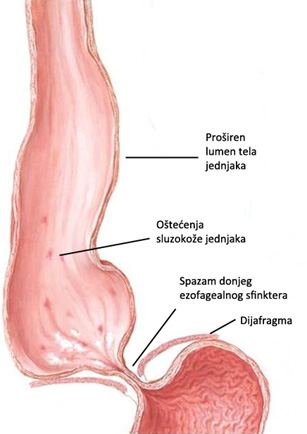
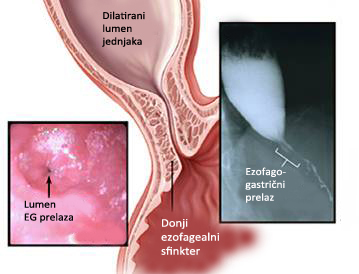
The act of swallowing (deglutition) normally begins perisaltički wave implemented by the food down the esophagus into the stomach.Deglutition is also activates the lower esophageal sphincter relaxations (DES), a process which ensures that swallowed food reaches the stomach.Normal DES relaxes every time you consume food in order to allow her to enter the normal stomach.When the food from the esophagus to the stomach muscles moved DES is aggregated to close the lower part of the esophagus, thus preventing stomach contents into the esophagus start (reflux).In patients with achalasia, during the act of swallowing DES is unable to normally relax (relax).Instead, the muscles DES continue to be in constant spasm (contraction) thus creating a kind of barrier that prevents food and liquid to pass to the stomach.Over time, the body of the esophagus above the constant spastic DES expands (dilates), and a greater amount of food, liquids or saliva, and are collected in the enlarged esophagus.
Achalasia is caused by damage to neurons in the wall of the esophagus that proudukuju nitric oxide (NO) and vasointestinal peptide (VIP), which directly affect the relaxation of DES.In some patients, degenerative changes are also found in the cells of the brain stem.Loss of innervation DES causes an increase in the basic pressure and impact on the sphincter muscle that is unable to properly relax.In the part of the smooth muscle of the body of the esophagus leads to the absence of peristaltic activity of the body of the esophagus (aperistaltika).The long achalasia often carries an increased risk of cancer of the esophagus pločastoslojevitog.
Although the primary etiology is not known achalasia, certain identifiable conditions can cause motor disturbance similar or identical to those of achalasia.This condition is called secondary achalasia or pseudoahalzija.The most important group of secondary diseases or pseudohalazije as Chagas’s disease and malignancies.The most common cause of secondary achalasia is a protozoal infection of Trypanosoma cruzi infection that leads to Chagas disease, which has its own endemic localization in Latin American countries.Malignancy can often be the cause pseudoahalazije.It is believed that in 160 patients with achalasia 6 occurs in patients with malignancies.This disease is significantly more common as older people, and five of the six patients basically have stomach cancer.In addition to gastric cancers, other tumors that may lead to pseudoahalazije are esophageal, lung, pancreas and or lymphomas.Other diseases that can have a similar clinical picture and motor disorders such as achalasia amyloidosis, sarcoidosis, neurofibromatosis, and eosinophilic gastroenteritis.
Symptoms
Long-term difficulty swallowing or dysphagia is the basic characteristic of achalasia, and patients often feel that they swallowed food or fluid retained behind the breastbone.Most patients with achalasia is presented progressive dysphagia for solids and liquids, although symptoms in its beginning may be subtle and nonspecific.This problem usually occurs gradually and over time gets worse.Most patients unfortunately not seek medical help for years, until the symptoms become very pronounced.The average duration of symptoms before the diagnosis of achalasia is approximately 2 years.The reason for this late diagnosis of patients with achalasia is usually inadequate recognition of clinical symptoms, so many patients are initially treated for other diseases, the most common gastroesophageal reflux disease.Some people compensate for their problems with swallowing by eating slowly and taking plenty of fluids during meals, and using a variety of maneuvers, such as raising the door or casting a shoulder in order to speed up easier swallowing food and liquids.

In patients with achalasia main symptom is dysphagia, which is often accompanied by varying degrees of spontaneous return of ingested food or liquids (regurgitation).Other symptoms of patients with achalasia may be a cough caused by aspiration (food or liquids entering the lungs), heartburn, chest pain, shortness of belching, fullness or lump in the throat of existence, as well as frequent hiccups, and all this is accompanied with weight loss .It has been shown that stressful conditions or taking cold liquids znčajno can aggravate symptoms achalasia.Regurgitation of undigested food in particular occurs after a meal or after occupying the supine position.As a result of regurgitation, aspiration of the contents of the esophagus can in about 10% of cases lead to bronchopulmonary complications.Many patients have a sense of mustard, which explains why some patients are initially misdiagnosed as GERD.Although patients with achalasia can have a gastro-oesophageal reflux, heartburn is much more often the result of the fermentation of undigested food in the esophagus.Chest pain occurs in more than 30% of patients, and its etiology is still unclear.The presence of pain is usually related to the existence of so-called.vigorously achalasia.
Fast onset of symptoms ( 50 years), or significant weight loss (> 10 kg) should arouse the suspicion of pseudoahalaziju, usually secondary to a malignant tumor.In these cases, in addition to the standard diagnostic approach is thoroughly examined with CT and / or endoscopic ultrasound before considering further treatment.
Diagnostic
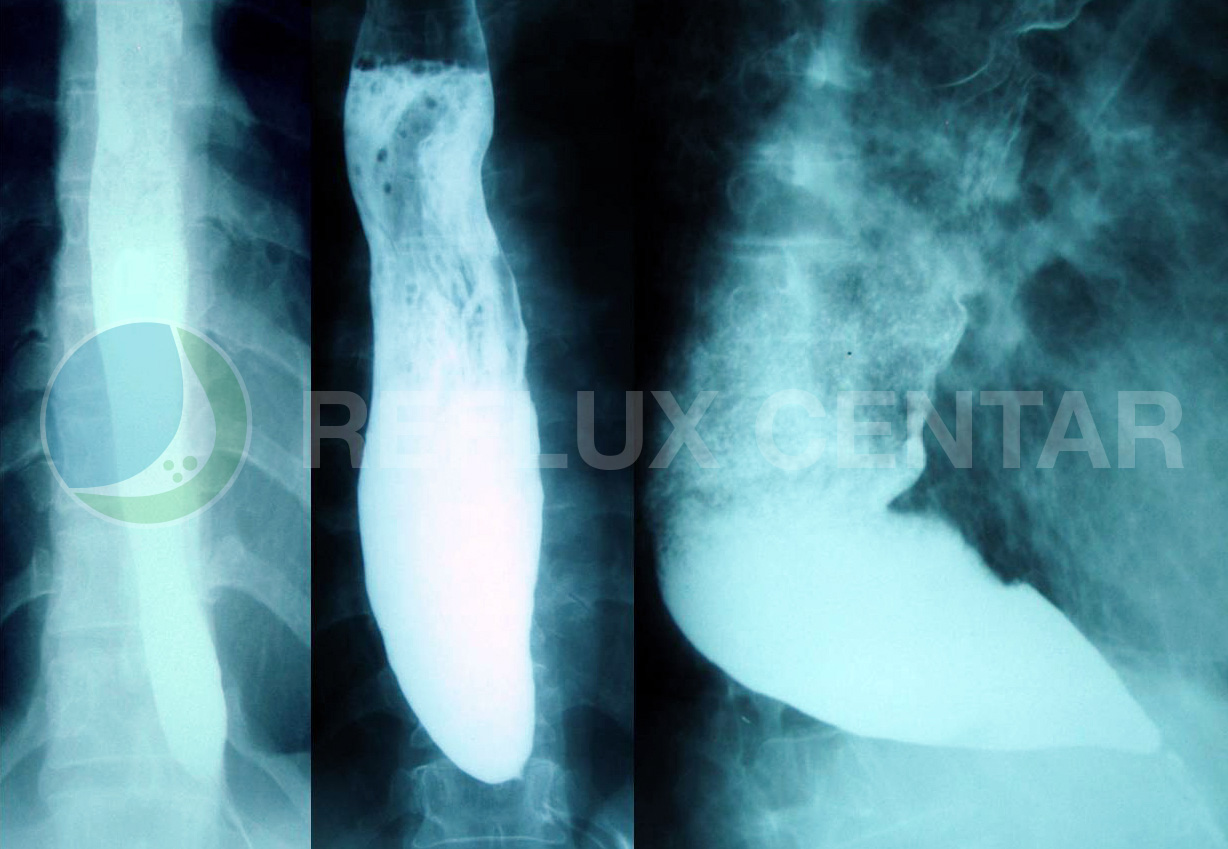
Barium radiography is usually the first diagnostic tool that is used in the assessment of dysphagia and may demonstrate liquid-gas levels in the esophagus with a lack of gastric air.The classic findings on chest radiograph barijumskoj the existence of so-called.”Bird beak” – narrowing of the distal esophagus with pole contrast in the lumen of the esophagus.There is an esophageal dilation variable, ranging from normal or mild (stage I incipient achalasia) in the early stages, significantly expanded via the esophagus (stage II dolihomegaezofagus) to massive (stage III sigmoid esophagus) forms the final stage.Radiographs may also reveal nepropulzivne, tertiary contractions of the esophageal body impossibility of “cleansing” barijumskog bolus from the distal esophagus.Sensitivity barijumskog tests, although higher than Endoscopy, is about 70%.
Endoscopic examination is always necessary and is used to rule out other processes that can mimic achalasia.Characteristic endoscopic findings of the esophagus has been expanded with the remains of food and fluids in the lumen, with no peristaltic contractions with firmly closed DES-player who does not open during insufflation (Air Injection).Gently pressing the endoscope, unlike peptic stricture or malignancy, passing through DES.Gastroesophageal junction, including the views of the cardoons from retroversion, should be carefully examined.
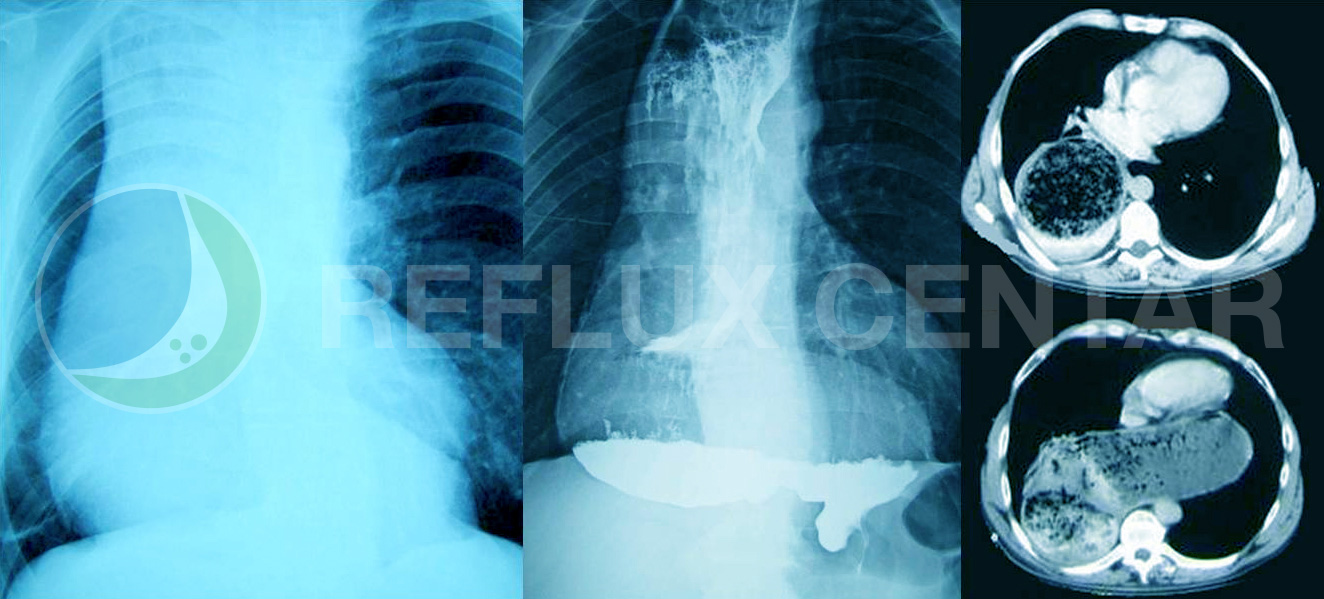
In some cases, especially in patients in stage III achalasia when there is a distinct dilatation radiographic presentation of sigmoid esophagus carcinoma is made and computed tomography (CT) to comprehend all aspects of organ grunod Recycle primarily in terms of damage to the lung parenchyma, and direct compression the surrounding organs.Patients with existence of sigmoid esophagus and chest radiography alone in the AP position be placed doubt on the existence of achalasia because of excessive dilation of the mediastinum especially the right side.
Manometry represents the “gold standard” to confirm the diagnosis of achalasia.Manometric characteristic necessary for the diagnosis of achalasia are ineffective (incomplete) or a time of smooth muscle relaxation of short-DES and after the act of swallowing, the increase in basal intraezofagealnog in relation to the pressure of the gastric and esophageal aperistaltika body, which is characterized by either simultaneous or nepropulzivnim kontrkcijama amplitude, or in general absence of esophageal contractions.Complete absence of peristalsis is in most cases a sure sign ahalazije.Ahalazija is based on manometry High Resolutions divided into three types.Type I achalasia involves the complete loss of esophageal peristalsis of the body, with impaired relaxation at the level of DES.With type II present panezofagealna pressurisation in at least 20% of the tested sip, while in type III achalasia present spasms in the body of the esophagus.Type II achalasia has the best and the worst type III response to therapy, whether it is a dilatation or surgical myotomy.
A special subgroup of patients present with frequent retrosternal pain and simultaneous contractions of the esophageal body of high amplitude (> 37 mmHg).This manometric labeled “vigorously achalasia”, and their differentiation from diffuse esophageal spasm can be achieved only by manometric examination.In both cases, radiographic examination can show the deformation of the esophagus as a “corkscrew” as well as the existence of diverticula.
Diseases
- Anatomy and Physiology of the Foregut
- Gastroesophageal Reflux Disease (GERD)
- Barrett’s Esophagus
- Hiatal Hernias
- Achalasia
- Esophageal Motility Disorders
- Esophageal Diverticula
- Helicobacter pylori gastritis
- Peptic Ulcer Disease (PUD)
- Gallstones (Cholelithiasis)
Lexicon
Patients Informations
Soon
You have Questions?
If you have more questions contact us:
info@refluxcentar.com
If you have more questions contact us:
info@refluxcentar.com